
Primary Liver Perivascular Epithelioid Cell Tumor (PEComa): Case Report and Literature Review

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
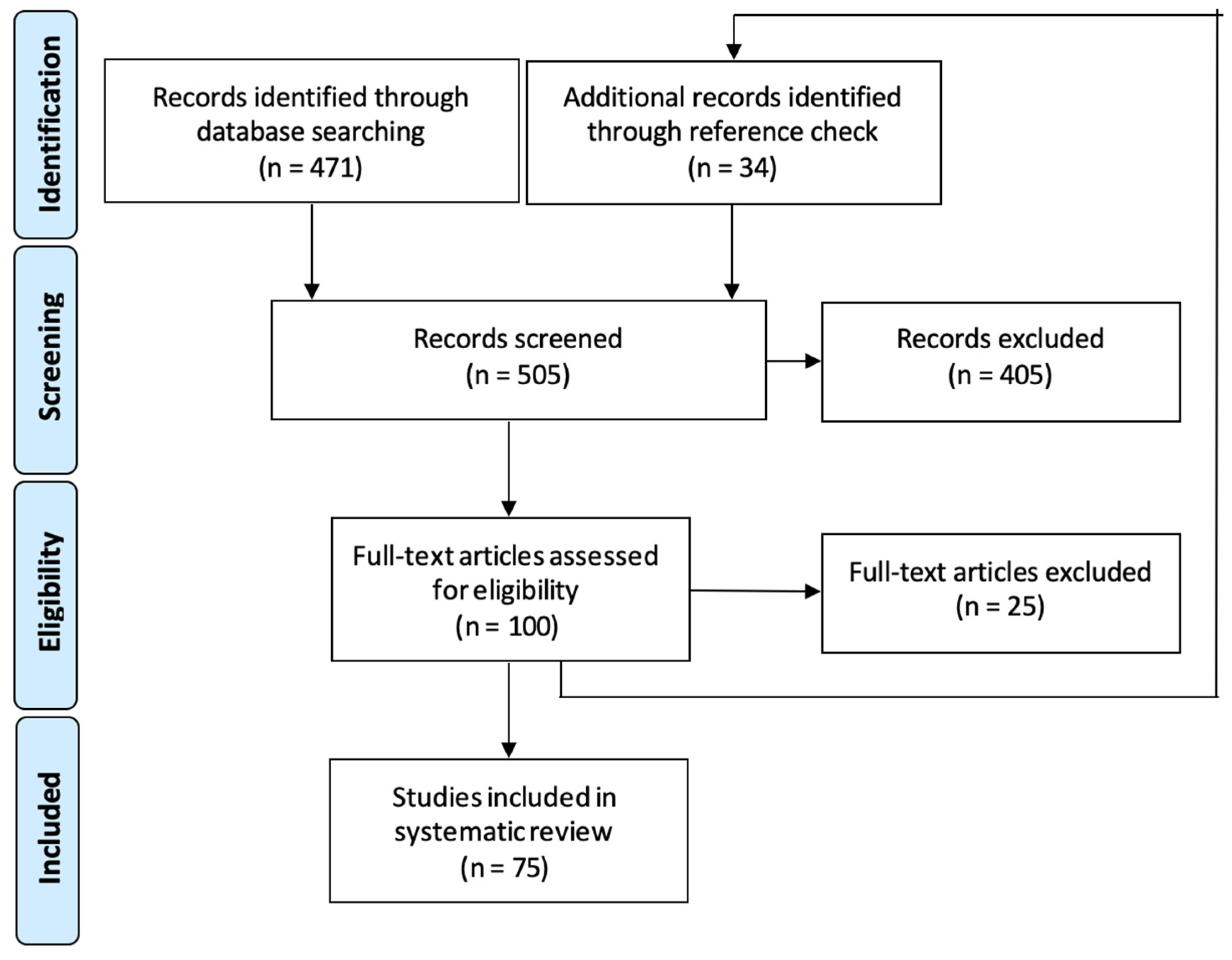
2. Materials and Methods
3. Case Report
4. Results of the Literature Review
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, D.; Shi, D.; Xu, Y.; Cao, L. Management of perivascular epithelioid cell tumor of the liver: A case report and review of the literature. Oncol. Lett. 2014, 7, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Bonetti, F.; Pea, M.; Martignoni, G.; Zamboni, G. PEC and sugar. Am. J. Surg. Pathol. 1992, 16, 307–308. [Google Scholar] [CrossRef] [PubMed]
- Maskoliūnaitė, V.; Jakubauskas, M.; Garnelytė, A.; Jotautas, V.; Stankevičienė, J.; Strupas, K.; Mickys, U. Rectal Perivascular Epithelioid Cell Tumor With Partial CD117 Expression and Giant Cells. AJSP Rev. Rep. 2020, 25, 189–194. [Google Scholar] [CrossRef]
- Giannella, L.; Delli Carpini, G.; Montik, N.; Verdecchia, V.; Puccio, F.; Di Giuseppe, J.; Tsiroglou, D.; Goteri, G.; Ciavattini, A. Ultrasound Features of a Uterine Perivascular Epithelioid Cell Tumor (PEComa): Case Report and Literature Review. Diagnostics 2020, 10, 553. [Google Scholar] [CrossRef]
- Hekimoglu, K.; Haberal, M. Liver Perivascular Epithelioid Cell Tumor with an Unusual Location: Diagnostic Characteristics with Multidetector Computed Tomography and Magnetic Resonance Imaging. J. Clin. Imaging Sci. 2017, 7, 36. [Google Scholar] [CrossRef] [PubMed]
- Kirste, S.; Kayser, G.; Zipfel, A.; Grosu, A.L.; Brunner, T. Unresectable hepatic PEComa: A rare malignancy treated with stereotactic body radiation therapy (SBRT) followed by complete resection. Radiat. Oncol. 2018, 13, 28. [Google Scholar] [CrossRef]
- Kiriyama, Y.; Tsukamoto, T.; Mizoguchi, Y.; Ishihara, S.; Horiguchi, A.; Tokoro, T.; Kato, Y.; Sugioka, A.; Kuroda, M. Intrahepatic peribiliary perivascular epithelioid cell tumor (PEComa) associated with heterotopic pancreas: A case report. Diagn. Pathol. 2016, 11, 81. [Google Scholar] [CrossRef]
- Fang, S.H.; Zhou, L.N.; Jin, M.; Hu, J.B. Perivascular epithelioid cell tumor of the liver: A report of two cases and review of the literature. World J. Gastroenterol. 2007, 13, 5537–5539. [Google Scholar] [CrossRef]
- Dalle, I.; Sciot, R.; de Vos, R.; Aerts, R.; van Damme, B.; Desmet, V.; Roskams, T. Malignant angiomyolipoma of the liver: A hitherto unreported variant. Histopathology 2000, 36, 443–450. [Google Scholar] [CrossRef]
- Han, X.; Sun, M.Y.; Liu, J.H.; Zhang, X.Y.; Wang, M.Y.; Fan, R.; Qamar, S. Computed tomography imaging features of hepatic perivascular epithelioid cell tumor: A case report and literature review. Medicine 2017, 96, e9046. [Google Scholar] [CrossRef]
- Bergamo, F.; Maruzzo, M.; Basso, U.; Montesco, M.C.; Zagonel, V.; Gringeri, E.; Cillo, U. Neoadjuvant sirolimus for a large hepatic perivascular epithelioid cell tumor (PEComa). World J. Surg. Oncol. 2014, 12, 46. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Yang, P.P.; Huang, Y.C.; Chen, H.C.; Chen, D.L.; Yan, W.T.; Yang, N.N.; Li, Y.; Li, N.; Feng, Z.Z. Hepatic perivascular epithelioid cell tumor: Clinicopathological analysis of 26 cases with emphasis on disease management and prognosis. World J. Gastroenterol. 2021, 27, 5967. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Wang, Q.; Zhou, X.; Zhou, H.; Jia, W.; Hu, C.; Chu, J.; Kong, L. Retrospective analysis of hepatic perivascular epithelioid cell tumour (PEComa) in a single centre for clinical diagnosis and treatment clinical diagnosis and treatment of hepatic PEComa. Medicine 2022, 101, e29506. [Google Scholar] [CrossRef]
- Zhou, Y.; Chen, F.; Jiang, W.; Meng, Q.; Wang, F. Hepatic epithelioid angiomyolipoma with an unusual pathologic appearance: Expanding the morphologic spectrum. Int. J. Clin. Exp. Pathol. 2014, 7, 6364–6369. [Google Scholar] [PubMed]
- Nie, P.; Wu, J.; Wang, H.; Zhou, R.; Sun, L.; Chen, J.; Yang, G. Primary hepatic perivascular epithelioid cell tumors: Imaging findings with histopathological correlation. Cancer Imaging 2019, 19, 32. [Google Scholar] [CrossRef] [PubMed]
- Maebayashi, T.; Abe, K.; Aizawa, T.; Sakaguchi, M.; Ishibashi, N.; Abe, O.; Takayama, T.; Nakayama, H.; Matsuoka, S.; Nirei, K.; et al. Improving recognition of hepatic perivascular epithelioid cell tumor: Case report and literature review. World J. Gastroenterol. 2015, 21, 5432–5441. [Google Scholar] [CrossRef] [PubMed]
- Holbrook, R.F.; Rodriguez-Bigas, M.A.; Ramakrishnan, K.; Blumenson, L.; Petrelli, N.J. Patterns of colorectal liver metastases according to Couinaud's segments. Dis. Colon Rectum 1995, 38, 245–248. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.Q.; Chen, D.F.; Sun, X.H.; Li, X.; Xu, J.; Hu, X.B.; Li, M.Q.; Wu, T.; Zhang, R.Y.; Li, K.Z. MRI diagnosis of perivascular epithelioid cell tumor (PEComa) of the liver. Rom. J. Morphol. Embryol. 2013, 54, 643–647. [Google Scholar]
- Parfitt, J.R.; Bella, A.J.; Izawa, J.I.; Wehrli, B.M. Malignant neoplasm of perivascular epithelioid cells of the liver. Arch. Pathol. Lab. Med. 2006, 130, 1219–1222. [Google Scholar] [CrossRef]
- Akitake, R.; Kimura, H.; Sekoguchi, S.; Nakamura, H.; Seno, H.; Chiba, T.; Fujimoto, S. Perivascular epithelioid cell tumor (PEComa) of the liver diagnosed by contrast-enhanced ultrasonography. Intern. Med. 2009, 48, 2083–2086. [Google Scholar] [CrossRef]
- Wang, Z.S.; Xu, L.; Ma, L.; Song, M.Q.; Wu, L.Q.; Zhou, X. Hepatic falciform ligament clear cell myomelanocytic tumor: A case report and a comprehensive review of the literature on perivascular epithelioid cell tumors. BMC Cancer 2015, 15, 1004. [Google Scholar] [CrossRef]
- Gennatas, C.; Michalaki, V.; Kairi, P.V.; Kondi-Paphiti, A.; Voros, D. Successful treatment with the mTOR inhibitor everolimus in a patient with perivascular epithelioid cell tumor. World J. Surg. Oncol. 2012, 10, 181. [Google Scholar] [CrossRef]
- O'Malley, M.E.; Chawla, T.P.; Lavelle, L.P.; Cleary, S.; Fischer, S. Primary perivascular epithelioid cell tumors of the liver: CT/MRI findings and clinical outcomes. Abdom. Radiol. 2017, 42, 1705–1712. [Google Scholar] [CrossRef]
- Tan, Y.; Xiao, E.H. Hepatic perivascular epithelioid cell tumor (PEComa): Dynamic CT, MRI, ultrasonography, and pathologic features--analysis of 7 cases and review of the literature. Abdom. Imaging 2012, 37, 781–787. [Google Scholar] [CrossRef] [PubMed]
- Folpe, A.L.; Mentzel, T.; Lehr, H.A.; Fisher, C.; Balzer, B.L.; Weiss, S.W. Perivascular epithelioid cell neoplasms of soft tissue and gynecologic origin: A clinicopathologic study of 26 cases and review of the literature. Am. J. Surg. Pathol. 2005, 29, 1558–1575. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, S.; Tanaka, S.; Fujii, H.; Matsumoto, T.; Okuda, C.; Watanabe, G.; Suda, K. Monotypic epithelioid angiomyolipoma of the liver. Histopathology 2000, 36, 451–456. [Google Scholar] [CrossRef]
- Tryggvason, G.; Blöndal, S.; Goldin, R.D.; Albrechtsen, J.; Björnsson, J.; Jónasson, J.G. Epithelioid angiomyolipoma of the liver: Case report and review of the literature. Apmis 2004, 112, 612–616. [Google Scholar] [CrossRef]
- Larbcharoensub, N.; Karnsombut, P.; Jatchavala, J.; Wasutit, Y.; Nitiyanant, P. Primary hepatic clear cell myomelanocytic tumor. Case report and review of the literature. Apmis 2007, 115, 1454–1459. [Google Scholar] [CrossRef]
- Della Vigna, P.; Preda, L.; Monfardini, L.; Gorone, M.S.; Maffini, F.A.; Bellomi, M. Growing perivascular epithelioid cell tumor of the liver studied with contrast-enhanced ultrasonography and magnetic resonance imaging. J. Ultrasound Med. 2008, 27, 1781–1785. [Google Scholar] [CrossRef] [PubMed]
- Paiva, C.E.; Moraes Neto, F.A.; Agaimy, A.; Custodio Domingues, M.A.; Rogatto, S.R. Perivascular epithelioid cell tumor of the liver coexisting with a gastrointestinal stromal tumor. World J. Gastroenterol. 2008, 14, 800–802. [Google Scholar] [CrossRef] [PubMed]
- Strzelczyk, J.M.; Durczynski, A.; Szymanski, D.; Jablkowski, M.; Dworniak, D.; Sporny, S. Primary perivascular epithelioid cell tumor (PEComa) of the liver: Report of a case. Surg. Today 2009, 39, 916–921. [Google Scholar] [CrossRef]
- Priola, A.M.; Priola, S.M.; Cataldi, A.; Marci, V.; Fava, C. Acute Abdomen as an Unusual Presentation of Hepatic PEComa: A Case Report. Tumori 2009, 95, 123–128. [Google Scholar] [CrossRef]
- Ahn, J.H.; Hur, B. Primary Perivascular Epithelioid Cell Tumor (PEComa) of the Liver-A Case Report and Review of the Literature. Korean J. Pathol. 2011, 45 (Suppl. S1), S93–S97. [Google Scholar] [CrossRef]
- Selvaggi, F.; Risio, D.; Claudi, R.; Cianci, R.; Angelucci, D.; Pulcini, D.; D’Aulerio, A.; Legnini, M.; Cotellese, R.; Innocenti, P. Malignant PEComa: A Case Report with Emphasis on Clinical and Morphological Criteria. BMC Surg. 2011, 11, 3. [Google Scholar] [CrossRef]
- Xie, L.; Jessurun, J.; Manivel, J.C.; Pambuccian, S.E. Hepatic Epithelioid Angiomyolipoma with Trabecular Growth Pattern: A Mimic of Hepatocellular Carcinoma on Fine Needle Aspiration Cytology. Diagn. Cytopathol. 2012, 40, 639–650. [Google Scholar] [CrossRef]
- Liu, Z.; Qi, Y.; Wang, C.; Zhang, X.; Wang, B. Hepatic Perivascular Epithelioid Cell Tumor: Five Case Reports and Literature Review. Asian J. Surg. 2012, 38, 58–63. [Google Scholar] [CrossRef]
- Yu, D.; Tang, S. Hepatic Perivascular Epithelioid Cell Tumor: A Case Report and Review of the Literature. Intern. Med. 2013, 52, 1333–1336. [Google Scholar] [CrossRef]
- Zhao, L.J.; Yang, Y.J.; Wu, H.; Huang, S.M.; Liu, K. Perivascular Epithelioid Cell Tumor of the Liver: A Case Report and Literature Review. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 1665–1668. [Google Scholar]
- Khaja, F.; Carilli, A.; Baidas, S.; Sriharan, A.; Norford, S. PEComa: A Perivascular Epithelioid Cell Tumor in the Liver—A Case Report and Review of the Literature. Case Rep. Med. 2013, 2013, 904126. [Google Scholar] [CrossRef] [PubMed]
- Patra, S.; Vij, M.; Kota, V.; Kancherla, R.; Rela, M. Pigmented Perivascular Epithelioid Cell Tumor of the Liver: Report of a Rare Case with Brief Review of Literature. J. Cancer Res. Ther. 2013, 9, 305–307. [Google Scholar] [CrossRef]
- Jafari, A.; Fischer, H.P.; von Websky, M.; Hong, G.S.; Kalff, J.C.; Manekeller, S. Primary Perivascular Epitheloid Cell Tumour (PEComa) of the Liver: Case Report and Review of the Literature. Z. Gastroenterol. 2013, 51, 1096–1100. [Google Scholar] [CrossRef]
- Cheung, T.T.; Trendell-Smith, N.; Poon, R.T. Primary Perivascular Epithelioid Cell Tumour (PEComa) of the Liver. BMJ Case Rep. 2013, 2013, bcr2013008706. [Google Scholar] [CrossRef]
- Tay, S.Y.; Lao, W.T.; Chen, C.L.; Chan, W.P. Contrast-Enhanced CT and Angiographic Findings in Hepatic Perivascular Epithelioid Cell Tumor. JBR-BTR 2013, 96, 308–310. [Google Scholar] [CrossRef]
- Ameurtesse, H.; Chbani, L.; Bennani, A.; Toughrai, I.; Beggui, N.; Kamaoui, I.; Elfatemi, H.; Harmouch, T.; Amarti, A. Primary Perivascular Epithelioid Cell Tumor of the Liver: New Case Report and Literature Review. Diagn. Pathol. 2014, 9, 149. [Google Scholar] [CrossRef] [PubMed]
- Khan, H.M.; Katz, S.C.; Libbey, N.P.; Somasundar, P.S. Hepatic PEComa: A Potential Pitfall in the Evaluation of Hepatic Neoplasms. BMJ Case Rep. 2014, 2014, bcr2014204122. [Google Scholar] [CrossRef] [PubMed]
- Abhirup, B.; Kaushal, K.; Sanket, M.; Ganesh, N. Malignant Hepatic Perivascular Epithelioid Cell Tumor (PEComa)-Case Report and a Brief Review. J. Egypt. Natl. Canc. Inst. 2015, 27, 239–242. [Google Scholar] [CrossRef] [PubMed]
- Hao, B.-B.; Rao, J.-H.; Fan, Y.; Zhang, C.-Y.; Dai, X.-Z.; Li, X.; Leng, Y.; Zhang, F. Hepatic Perivascular Epithelioid Cell Tumor in Three Patients. Hepatobiliary Pancreat. Dis. Int. 2016, 15, 660–664. [Google Scholar] [CrossRef] [PubMed]
- Tang, D.; Wang, J.; Tian, Y.; Li, Q.; Yan, H.; Wang, B.; Xiong, L.; Li, Q. Hepatic Perivascular Epithelioid Cell Tumor: Case Report and Brief Literature Review. Medicine 2016, 95, e5572. [Google Scholar] [CrossRef] [PubMed]
- Lan, Y.Z.; Hua, X.E. Hepatic Multiple Perivascular Epithelioid Cell Neoplasm: A Case Report and Literature Review. Mol. Clin. Oncol. 2016, 4, 619–621. [Google Scholar] [CrossRef]
- Schaeffer, D.F.; Poulin, M.P. Primary Hepatic Perivascular Epithelioid Tumor (PEComa). Ann. Hepatol. 2016, 15, 436–437. [Google Scholar] [CrossRef]
- Son, H.J.; Kang, D.W.; Kim, J.H.; Han, H.Y.; Lee, M.K. Hepatic Perivascular Epithelioid Cell Tumor (PEComa): A Case Report with a Review of Literatures. Clin. Mol. Hepatol. 2017, 23, 80–86. [Google Scholar] [CrossRef]
- Chen, W.; Liu, Y.; Zhuang, Y.; Peng, J.; Huang, F.; Zhang, S. Hepatic Perivascular Epithelioid Cell Neoplasm: A Clinical and Pathological Experience in Diagnosis and Treatment. Mol. Clin. Oncol. 2017, 6, 487–493. [Google Scholar] [CrossRef]
- Guan, H.; Zou, Y.; Lv, Y.; Wang, C. Hepatic Perivascular Epithelioid Cell Tumor Treated by Transarterial Embolization Plus Radiofrequency Ablation: A Case Report and Literature Review. Medicine 2017, 96, e6969. [Google Scholar] [CrossRef]
- Cardoso, H.; Silva, M.; Vilas-Boas, F.; Cunha, R.; Lopes, J.; Maia, J.C.; Macedo, G. Hepatic Perivascular Epithelioid Tumor (PEComa). A Case Report. Clin. Res. Hepatol. Gastroenterol. 2017, 41, e43–e46. [Google Scholar] [CrossRef] [PubMed]
- Otegi Altolagirre, I.; de Miguel Valencia, M.; Sánchez Acedo, P.; Zazpe Ripa, C.; Tarifa Castilla, A.; Herrera Cabezón, J.; Gómez Dorronsoro, M.; Jiménez Mendioroz, J. Our Experience in the Surgical Treatment of Liver PEComa. Gastroenterol. Y Hepatol. (Engl. Ed.) 2017, 40, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Huang, P.; Gao, H.; Zhai, W. Hepatic Perivascular Epithelioid Cell Tumor (PEComa): Analyses of 13 Cases and Review of the Literature. Int. J. Clin. Exp. Pathol. 2018, 11, 2759–2767. [Google Scholar] [PubMed]
- Dezman, R.; Masulovic, D.; Popovic, P. Hepatic Perivascular Epithelioid Cell Tumor: A Case Report. Eur. J. Radiol. Open 2018, 5, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Kirnap, M.; Ozgun, G.; Moray, G.; Haberal, M. Perivascular Epithelioid Cell Tumor Outgrowth from the Liver. Int. J. Surg. Case Rep. 2018, 53, 295–298. [Google Scholar] [CrossRef] [PubMed]
- Voulgari, P.V.; Tatsi, V.; Milionis, H.J.; Goussia, A.; Xydis, V.; Glantzounis, G.K. Liver Perivascular Epithelioid Cell Tumor in a Patient with Systemic Lupus Erythematosus. Int. J. Surg. Case Rep. 2018, 53, 193–195. [Google Scholar] [CrossRef]
- Lopes, C.V.; Goldoni, M.B.; Barra, M.B.; Hartmann, A.A.; Artifon, E.L.A. Pedunculated Hepatic Angiomyolipoma: A Rare Entity. Presse Med. 2019, 48, 1189–1190. [Google Scholar] [CrossRef]
- Kiuchi, R.; Sakaguchi, T.; Kitajima, R.; Furuhashi, S.; Takeda, M.; Hiraide, T.; Morita, Y.; Ushio, T.; Ishikawa, R.; Baba, S.; et al. Hepatic Angiomyolipoma with Early Drainage Veins into the Hepatic and Portal Vein. Clin. J. Gastroenterol. 2019, 12, 361–366. [Google Scholar] [CrossRef]
- Li, Y.; Zeng, K.N.; Ruan, D.Y.; Yao, J.; Yang, Y.; Chen, G.H.; Wang, G.S. Feasibility of Laparoscopic Isolated Caudate Lobe Resection for Rare Hepatic Mesenchymal Neoplasms. World J. Clin. Cases 2019, 7, 3194–3201. [Google Scholar] [CrossRef]
- Chai, V.; Fox, A.; Chong, L.; House, E.; Sutherland, T. Contrast-Enhanced Sonographic Appearances of Two Primary Hepatic Epithelioid Angiomyolipomas. J. Clin. Ultrasound. 2020, 48, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Xu, H.; Yang, H.; Du, S.; Mao, Y. Primary Hepatic Perivascular Epithelioid Cell Neoplasm (PEComa) with Fever in a 53-Year-Old Man. Postgrad. Med. J. 2020, 96, 505–506. [Google Scholar] [CrossRef] [PubMed]
- Galera Lopez, M.D.M.; Marquez Rodas, I.; Agra Pujol, C.; Garcia Perez, A.; Velasco Sanchez, E.; Alvarez Alvarez, R. Simultaneous Diagnosis of Liver PEComa in a Family with Known Li-Fraumeni Syndrome: A Case Report. Clin. Sarcoma Res. 2020, 10, 24. [Google Scholar] [CrossRef] [PubMed]
- Nakra, T.; Das, P.; Gupta, B.; Yadav, R.; Singh, A.N.; Dash, N.R.; Madhusudhan, K.S.; Ramteke, P. Primary Multifocal Hepatic PEComa: A Rarely Encountered Diagnostic Dilemma. J. Gastrointest. Cancer 2020, 51, 667–672. [Google Scholar] [CrossRef] [PubMed]
- De la Sancha, C.; Khan, S.; Alruwaii, F.; Cramer, H.; Saxena, R. Hepatic Angiomyolipoma with Predominant Epithelioid Component: Diagnostic Clues on Aspiration and Core Needle Biopsies. Diagn. Cytopathol. 2021, 49, E238–E241. [Google Scholar] [CrossRef]
- Mochizuki, K.; Aoki, T.; Kusano, T.; Tomioka, K.; Tashiro, Y.; Koizumi, T.; Matsuda, K.; Enami, Y.; Yamochi, T.; Murakami, M. Laparoscopic Resection of a Hepatic Epithelioid Angiomyolipoma Revealed by Indocyanine Green Fluorescence Imaging. Am. Surg. 2023, 89, 2061–2063. [Google Scholar] [CrossRef]
- Huang, Z.; Xin, J.Y.; Li, K.Y. Ultrasound Contrast Agent Sonazoid for the Diagnosis of Hepatic Epithelioid Angiomyolipoma: A Case Report. BMC Gastroenterol. 2021, 21, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Wang, G.; Sun, G.; Xie, B.; Xiao, W.; Li, Y. Primary hepatic epithelioid angiomyolipoma: A small case series. ANZ J. Surg. 2022, 92, 1803–1808. [Google Scholar] [CrossRef]
- Wang, S.; Xia, H.; Liu, X.; Liu, Y.; Cen Lou, M.D. Hepatic epithelioid angiomyolipoma mimicking hepatocellular carcinoma on MR and F-FDG PET/CT imaging: A case report and literature review. Hell. J. Nucl. Med. 2022, 25, 205–209. [Google Scholar]
- Chai, J.; Ma, J.; Liu, Y.; Zhao, D.; Yin, Z.; Wang, Z.; Fan, L. ASPSCR1-TFE3 fusion in a case of Xp11 translocation PEComa of the liver: Are ASPSCR1-TFE3 fusion-bearing tumours Xp11 translocation PEComa or alveolar soft part sarcoma? Pathology 2023, 55, 416–419. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, T.; Sasaki, T.; Takahashi, Y.; Takamatsu, M.; Kanda, H.; Hiratsuka, M.; Matsuyama, M.; Ozaka, M.; Sasahira, N. Perivascular epithelioid cell tumor (PEComa) of the cystic duct. Clin. J. Gastroenterol. 2023, 16, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.; Sun, S.; Deng, Y.; Liu, J.; Pan, S. Hepatic epithelioid angiomyolipoma is scattered and unsuitable for surgery: A case report. J. Int. Med. Res. 2023, 51, 03000605231154657. [Google Scholar] [CrossRef]
- Matrood, S.; Görg, C.; Safai Zadeh, E.; Alhyari, A. Hepatic perivascular epithelioid cell tumor (PEComa): Contrast-enhanced ultrasound (CEUS) characteristics—A case report and literature review. Clin. J. Gastroenterol. 2023, 16, 444–449. [Google Scholar] [CrossRef] [PubMed]
- Velasco-Albendea, F.J.; Gil-Belmonte, M.J.; Estébanez-Ferrero, B.; Fuentes-Porcel, O.; Nievas-Soriano, B.J. A case report of hepatic angiomyolipoma, inflammatory subtype. Clinico-pathological characterization: A diagnostic challenge. Diagn. Pathol. 2023, 18, 1–9. [Google Scholar] [CrossRef]
- Kou, Y.Q.; Yang, Y.P.; Ye, W.X.; Yuan, W.N.; Du, S.S.; Nie, B. Perivascular epithelioid cell tumors of the liver misdiagnosed as hepatocellular carcinoma: Three case reports. World J. Clin. Cases 2023, 11, 426. [Google Scholar] [CrossRef]
- Dhaliwal, K.; Marslender, S. Malignant retroperitoneal PEComa: A case report with emphasis on radiological findings. Radiol. Case Rep. 2023, 18, 1358–1363. [Google Scholar] [CrossRef]
- Harwal, R.; Rosemary, L.J.; Raju, P.; Chidambaranathan, S.; Jayanthi, J.B.; Lakshmanamoorthy, N.B. Hepatic Perivascular Epithelioid Cell Tumor Mimicking Hepatocellular Carcinoma. ACG Case Rep. J. 2023, 10, e00962. [Google Scholar] [CrossRef]
- Yazıcı, C.; Gündoğdu, E. Very Rare Liver Tumor: PEComa Case Report with and a Review of Literature. Indian J. Radiol. Imaging 2023, 34, 172–176. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Marker | Positive Cells (%) |
|---|---|
| Melanocytic markers | |
| HMB45 | 100 |
| Melan-A/MART1 | 30 |
| MiTF | - |
| S100 | - |
| TFE3 | - |
| Smooth muscle markers | |
| SMA | 100 |
| Desmin | 60 |
| H-caldesmon | 90 |
| Other markers | |
| CD68 | 100 |
| CD117 | Several |
| DOG1 | - |
| Ki67 | <1 |
| Parameter | Value |
|---|---|
| Patient characteristics | |
| Female sex, n (%) | 178 (79.5%) |
| Mean age (years) | 45.3 |
| Continent of publications | |
| Asia, n (%) | 46 (61.3%) |
| Europe, n (%) | 19 (25.3%) |
| North America, n (%) | 7 (9.3%) |
| South America, n (%) | 1 (1.3%) |
| Africa, n (%) | 1 (1.3%) |
| Australia, n (%) | 1 (1.3%) |
| Manifestation | |
| Abdominal pain, n (%) | 53 (50.0%) |
| Discomfort, n (%) | 35 (33.0%) |
| Nausea, n (%) | 7 (6.6%) |
| Tumor characteristics | |
| Average size (mm) | 71.2 |
| Min | 13.0 |
| Max | 300.0 |
| Single nodule, n (%) | 211 (94.2%) |
| Multi-nodule, n (%) | 13 (5.8%) |
| RL, n (%) | 126 (56.0%) |
| LL, n (%) | 91 (40.4%) |
| CL, n (%) | 6 (2.7%) |
| Treatment modalities | |
| Biopsy, n (%) | 45 (20.1%) |
| Surgery, n (%) | 183 (81.3%) |
| Arterial chemoembolization, n (%) | 3 (1.3%) |
| Adjuvant treatment, n (%) | 4 (1.8%) |
| Neoadjuvant treatment, n (%) | 3 (1.3%) |
| Surveillance, n (%) | 19 (8.4%) |
| Immunohistochemistry | |
| HMB45, n (%) | 193/193 (100.0%) |
| Melan-A, n (%) | 156/158 (98.7%) |
| S100, n (%) | 50/78 (64.1%) |
| SMA, n (%) | 130/144 (90.3%) |
| Desmin, n (%) | 40/67 (59.7%) |
| H-caldesmon, n (%) | 2/5 (40.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kvietkauskas, M.; Samuolyte, A.; Rackauskas, R.; Luksaite-Lukste, R.; Karaliute, G.; Maskoliunaite, V.; Valkiuniene, R.B.; Sokolovas, V.; Strupas, K. Primary Liver Perivascular Epithelioid Cell Tumor (PEComa): Case Report and Literature Review. Medicina 2024, 60, 409. https://doi.org/10.3390/medicina60030409
Kvietkauskas M, Samuolyte A, Rackauskas R, Luksaite-Lukste R, Karaliute G, Maskoliunaite V, Valkiuniene RB, Sokolovas V, Strupas K. Primary Liver Perivascular Epithelioid Cell Tumor (PEComa): Case Report and Literature Review. Medicina. 2024; 60(3):409. https://doi.org/10.3390/medicina60030409
Chicago/Turabian StyleKvietkauskas, Mindaugas, Austeja Samuolyte, Rokas Rackauskas, Raminta Luksaite-Lukste, Gintare Karaliute, Vygante Maskoliunaite, Ruta Barbora Valkiuniene, Vitalijus Sokolovas, and Kestutis Strupas. 2024. "Primary Liver Perivascular Epithelioid Cell Tumor (PEComa): Case Report and Literature Review" Medicina 60, no. 3: 409. https://doi.org/10.3390/medicina60030409