Unit 2: Protozoa
6
Lecture 1+2+3+4+5 –
Subphylum Sarcodina (Amoeba)
Classification
Subkingdom: Protozoa
Phylum: Sarcomastigophora
a. Subphylum: Sarcodina
b. Subphylum: Mastigophora
Phylum: Ciliophora
Phylum: Apicomplexa
Amoeba
Phylum: Sarcomastigophora
Subphylum: Sarcodina
Superclass: Rhizopoda
Class: Lobosea
General characters of Amoeba
All the members move by pseudopodium.
Having Trophozoite stage.
Multiplication by binary division.
Some of them parasitic, other free living.
Generic classification depends on structures of nuclear
contents.
Commonly parasitizing the large intestine of man, except
Entamoeba gingivalis, which parasitized the oral cavity.
Members of this family are:
1) Entamoeba histolytica
2) Entamoeba hartmani
3) Entamoeba coli
4) Entamoeba gingivalis
5) Endolimax nana
6) Iodamoeba buetschlii
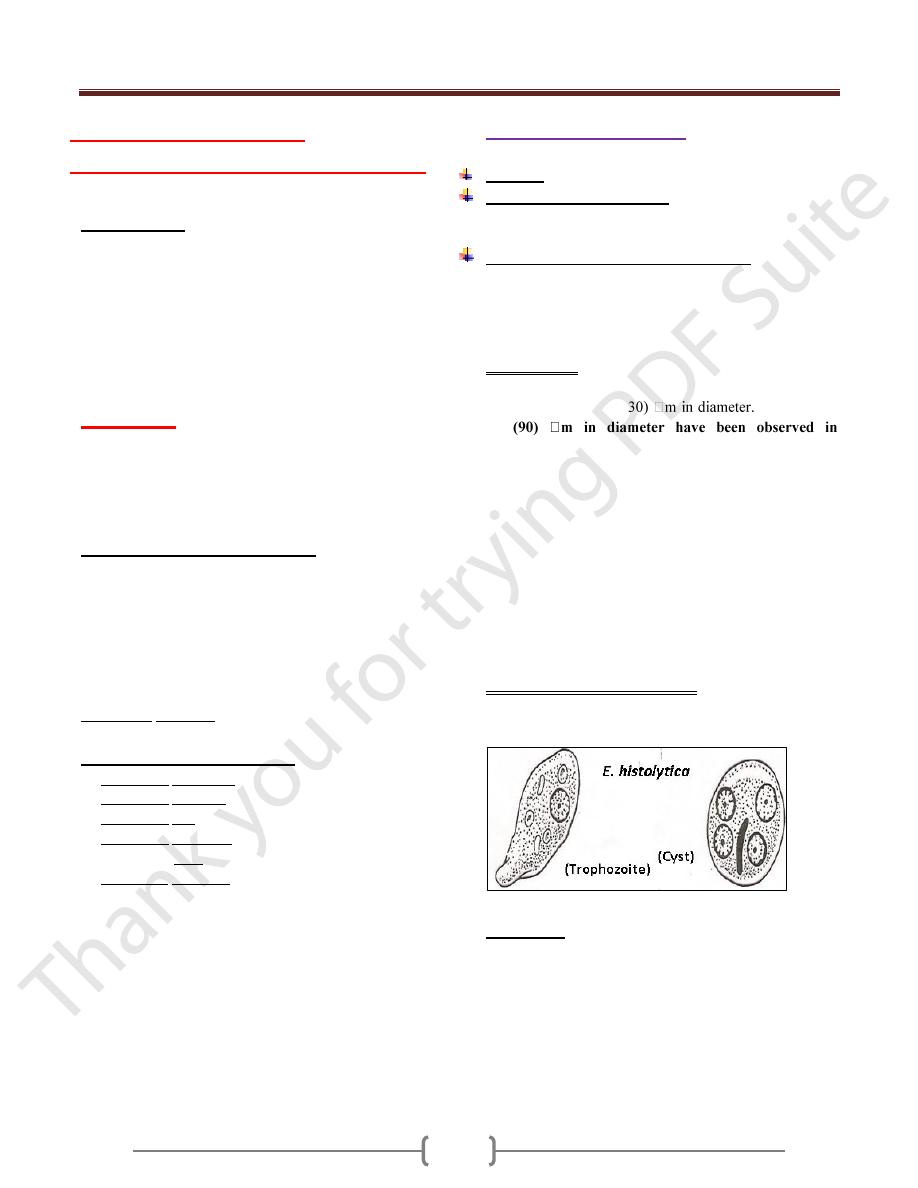
Entamoeba histolytica
Disease:
Amebiasis
Geographical distribution
Cosmopolitan mainly in tropical & subtropical area.
Morphology, Biology & Life cycle:
It has four stages: Trophozoite, precyst, cyst, metacyst
The stages recognized in the feces are trophozoites &
cysts. The other two found only inside the host body
(precyst, metacyst)
Trophozoite:
In its natural habitat, the large intestine & extra intestinal
foci the size about (12-
Trophozoite
up
dysenteric stools.
Trophozoite has finely granular, endoplasm & a clear,
grayish, green tinge ectoplasm.
The endoplasm contain many structures include nucleus &
food vacuoles within the food vacuoles we may see RBC.
The nucleus spherical, surrounded by delicate nuclear
membrane which on its inner surface there is fine,
regularly distributed chromatin granules.
In the center of the nucleus there is single dense
karyosome. Immediately around the karyosome there is
clear halo extending between this & the nuclear
membrane are radially exending a chromatin fibrils.
The pseudopodia have 2 types
1) Lobopodia: for the locomotion
2) Filopodia: for attachment to cells
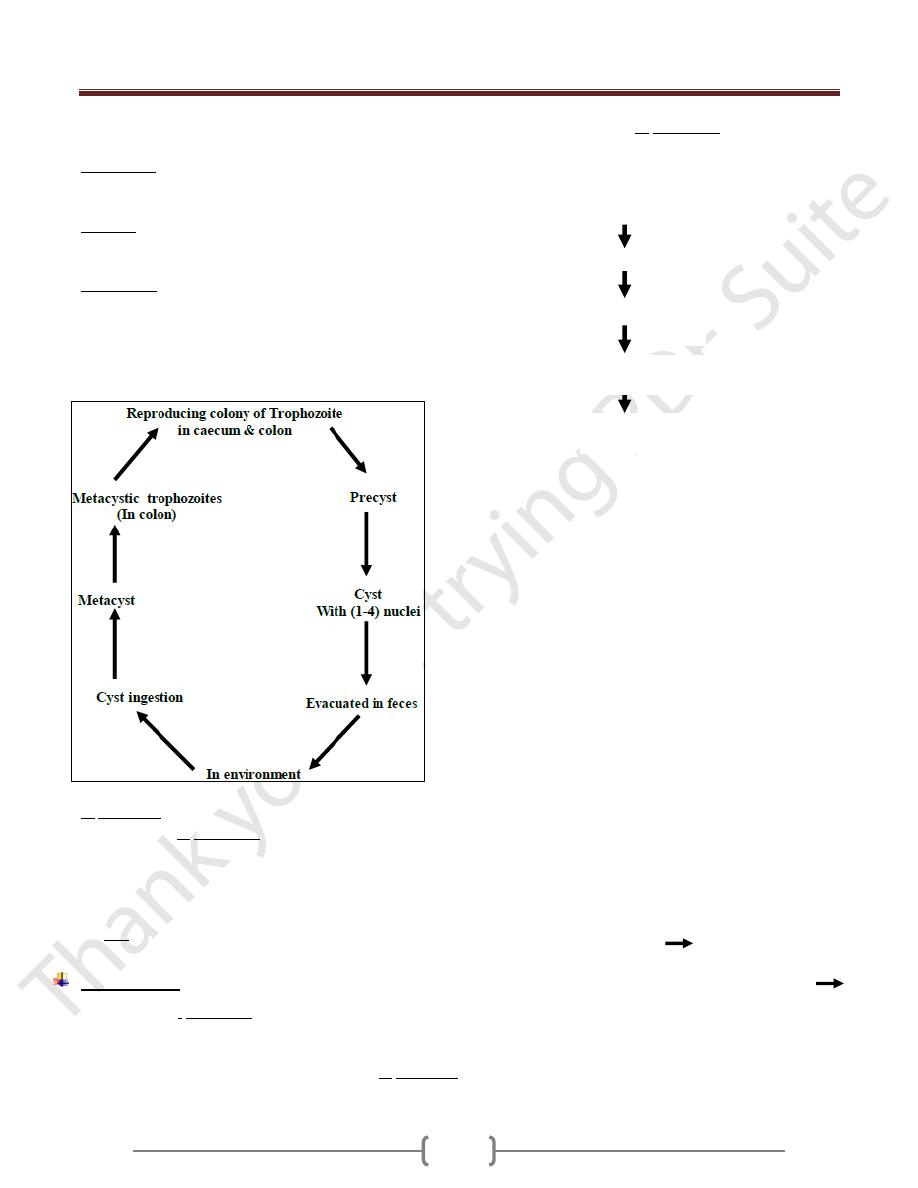
Life Cycle
Trophozoite stage convert to precyst stage which convert
to cyst stage with mononucleus, this divided into 2
nuclei, then these 2 nuclei will divide into 4 nuclei which
now called mature cyst.
The infection is usually started with the cyst stage by
contaminated food or water ingested by man. The cyst
usually not affected by the juice of stomach.
Unit 2: Protozoa
7
When it goes to or through intestine it under go 3
processes which are:
a) Excystation: Means the liberation of the metacyst from
cyst wall, then the cytoplasm divided forming metacystic
trophozoites. So after that 4 trophozoites are formed.
b) Invasion: The trophozoite invades the wall of large
intestine, particularly the caecum & colon & then
colonization results from multiplication by binary division.
c) Encystation: Occur in the large intestine, when the
Trophozoite dehydrated in bowel lumen, encystation
started.
Trophozoite, precyst considered as diagnostic stage.
Mature cyst as infective stage.
E. histolytica habitat is Caecum & flexure colon.
Viable cysts of E. histolytica in external environment are
soon killed by drying, direct sun light, heat, hypertonicity
& bacterial putrefaction.
Cyst passed in semiformed, form, solid, semisolid stool.
Trophozoite & precyst dies rapidly (so non-infective)
but cyst is resistance (infective stage).
Pathogenesis
Infection with E. histolytica leads to formation of
colonization.
The speed & depth of penetration depends on:
Pathogenic capacity of the particular strain of E. histolytica
General resistance of the host.
The damage caused by E. histolytica is:
1) Chemical (Enzyme action)
2) Mechanical (engulfing of the parasite)
Trophozoite may lodge in the crypts of large intestine
Lesion result from invasion leading to superficially
minute cavity (are result of lytic necrosis of the parasite
on colon mucosa).
More colonizing & more lytic action leading to narrow
channel, which lead to base of the mucosa.
The invasion extend laterally which leads to Flask
shaped ulcer, and the repair may take place to lytic
necrosis, lesion leads to extensive functional damage to
the mucosa.
In many cases, the Amoeba erode a passage into
muscularis mucosa then sub mucosa.
It can spread radially to surrounding tissues. (If there is
no secondary bacterial infection, there is no tissue
reaction).
From submucosa, the invasion extends to muscular coats
& penetrate to serosa (Perforation). It may perforate
mesenteric venules or lymphatics & carried into the liver
& other extraintestinal sites (brain, lung).
Any extraintestinal lesion is secondary to primary lesion
in large intestine except cutaneous lesion of the genitalia.
So the early uncomplicated amebic lesions are minute
opening with slightly raised yellowish ring in mucosa
leading into a deeper enlargement in the submucosa with
tunneled connection between two or more lesions leading
to cuts off the blood supply sloughing of overlying
layers.
As the lesion becomes chronic by bacterial infection
tissue reaction & cell infiltration, with neutrophilic
leukocytes & fibroblasts tend to form a wall around the
ulcer & over hanging edges become thickened.
Feeding
Colonized
Lytic activity
Invasion
Unit 2: Protozoa
8
Extraintestinal amebic lesion
At first consists of a small lesion where are a more ameba
enter the blood vessels & lodged into the liver or other
organ proceed to colonize producing necrosis of
surrounding host cells.
In the liver, tendency for lesion to be multiple-later one or
at most few become enlarged to develop amebic liver
abscess, this lesion bacteriologicaly sterile, but the
amount of tissue necrosis stimulates local & systemic
Leukocytosis.
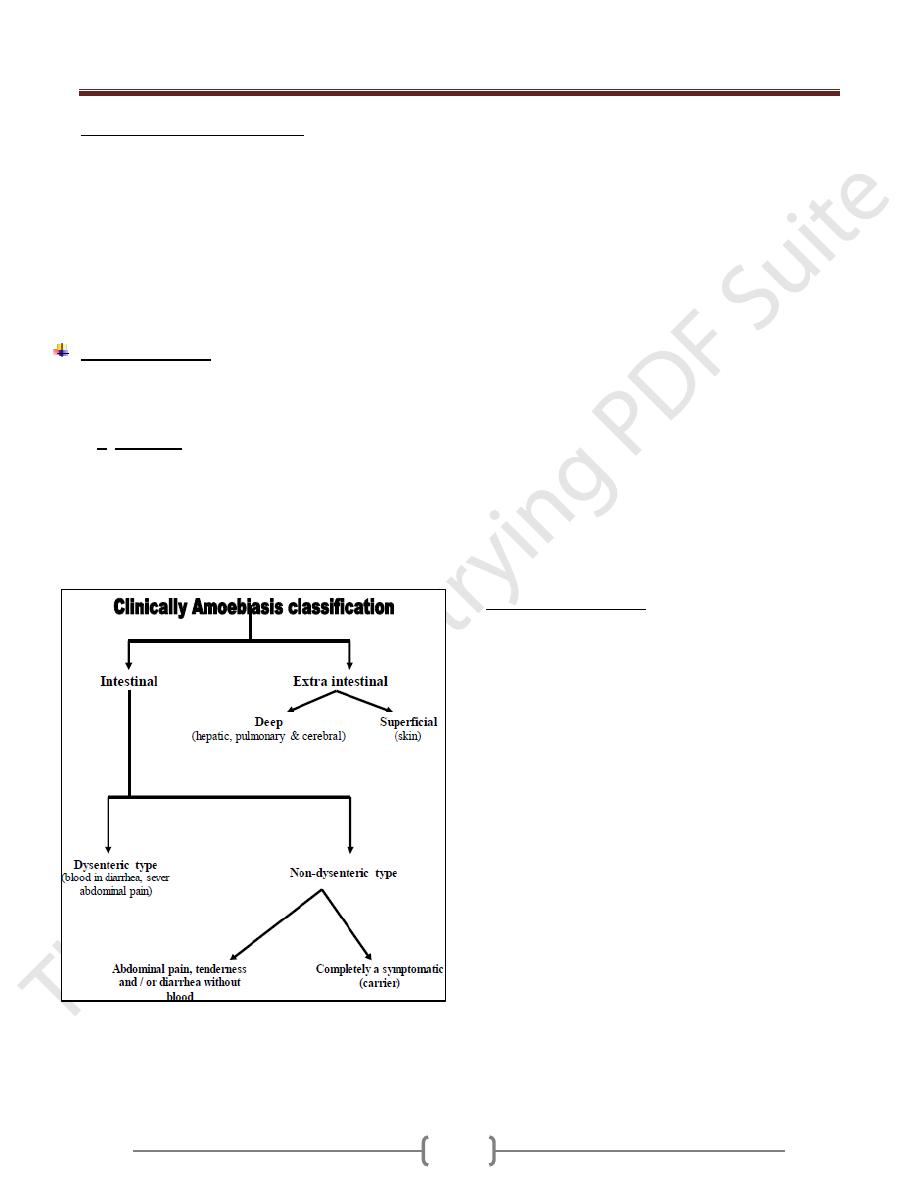
Symptomatology
The incubation period (the time or duration from time of
exposure till first symptoms appears) is varying from few
days to 3 months or even a year.
In E. histolytica it is difficult to determine the interval
between exposure & first symptoms. The onset may be
insidious with vague (not sharp) abdominal discomfort or
soft stools for variable period or it may be sudden with
dysentery or acute abdominal pain.
In hepatic amebiasis, frequently there is no history of
amebic infection in colon.
Amebiasis may be only one of two or more concurrent
disease processes, example, Shigellosis, Salmonellosis,
carcinoma, appendicitis, peptic ulcers, cholecystitis.
At time or more amoebic granulomas (amebomas)
develop in the wall of colon or rectum.
The patient with amebic dysentery has tenesmus,
abdominal cramps. No systemic intoxication as seen in
bacillary dysentery.
The abdominal pain & tenderness are mostly in the lower
quadrants of the abdomen, on the right side. Clinically
sometime mistaken for appendicitis.
Extraintestinal symptoms depend on the organ affected.
Hepatic abscess presents with fever, enlarged tender are
mostly in the lower quadrants of the abdomen, on the
right side, clinically sometimes mistaken for appendicitis.
Extraintestinal symptoms depend on the organ affected.
Hepatic abscess present with fever, enlarged tender liver,
bulging & fixation of the right leaf of the diaphragm &
serious effusion of the right pleura.
Skin amoebiasis occurs due to damaged skin come in
contact with trophozoite stage.
Most common skin infection seen in:
1) Perineum, secondary to amoebic dysentery.
2) Penile lesion, acquired by anal intercourse.
3) The abdomen, at the mouth of fistulous tract from
colon or from hepatic abscess.
Pulmonary amoebiasis
Is a consequence of rupture of hepatic abscess into the
chest cavity, the lung & the bronchus. Therefore, the
patient present with signs of pneumonia & expectoration
of characteristic bitter, bile flavored liver-colored pus
passing through the hepatobronchial fistula
Rarely, amoebic lung abscess occurs by hematogenous
spread from the colon.
The amoeba secrete proteolytic enzymes that produce
necrosis of tissue & steps involved in amoebic killing the
target cell are:
1) Receptor mediated adherence of Entamoeba to target cell
2) Amoeba cytolysis of target cells
3) Amoebic phagocytosis of killed as viable target cells.
Attachment of Entamoeba histolytica to mucosa mediated
by amoebal galactose-inhibatable adherence Lectin.
Colonization of E. histolytica depends on:
1) Normal motility of intestine.
2) Proper establishment of metabolic requirements
3) Infected dose
4) Adequate bacterial flora.
5) Low oxygen tension
6) PH
In the cecum sometime, adjacent ulcers caused by
E.hitolytica may coalesce causing sloughing of
Unit 2: Protozoa
9
intervening mucosa to form the typical Dyak hair ulcer as
buffalo skin ulcer.
Factors determining development of amoebiasis:
1) Strain variation
2) Role of bacteria
3) Infective dose
4) Nutritional status
5) Associated disease (such as diabetes, tuberculosis &
malignancy), pregnancy
6) Immunity
7) Intestinal mucus
Complications of intestinal amoebiasis:
Local complication: Perforations, peritonitis, prolapse of
rectum, hemorrhage & obstruction stricture
Systemic complications: hepatic amoebiasis, pulmonary
amoebiasis, cerebral amoebiasis, splenic amoebiasis &
cutaneous amboebiasis
Amoebic liver abscess
Early stages appear homogenous area of yellow color
surrounded by zone of hemorrhagic liver tissue & nicrotic
material thick.
In advance cases, liquefaction of the central necrotic area
with cavitation may be visible. The abscess gives honey-
comb appearance as the connective tissue is more
resistant to liquefaction.
The pus on the cavity is thick fluid whose color may vary
greyish-yellow to chocolate & it is called anchovy sause-
like pus.
Microscopically, the pus reveals degenerated liver cells,
RBCs, WBCs & bacteriologically sterile.
Microscopic pathology to of amoebic liver abscess:
In a section passing through the margins of the liver
abscess. There are 3 zones can be differentiated:
1) Central zone of cytolysed material with no amoeba.
2) Intermediate area consisting of degenerated liver cells,
RBCs, WBCs, connective tissue & occasionally
trophozoites of E.histolytica
3) A peripheral zone consisting of congested capillaries with
necrotic liver cells with many trophozoite of E.histolytica
Diagnosis
Intestinal amoebiasis cannot be diagnosed on clinical
ground only, primary depend on direct microscopic
examination of the stool to recover motile trophozoite &
charcot-leyden crystals.
In extra intestinal amoebiasis, routine work of
Histopathology using (Best’s carmine) stain must be perform
Treatment
Depend on clinical type. In severe amebic dysentery the
purpose of treatment is not only to provide relief of
discomfort but also improve eradication of amebic infection.
Intestinal amoebiasis, the drug of choice is
Metronidazole 750 mg, Tid for (5-10) days.
Diiodohydroxyquin.
Antibiotic (Tetracycline).
Emetine hydrochloride, also effective.
Non dysenteric symptoms:
Diloxanide furoat & Diiodohydroxyquin.
A symptomatic cases:
Must be treated by Metronidazole.
Extraintestinal:
Metronidazole.
Emetin hydrochloride.
Chloroquine.
Or all of them
Epidemiology
High prevalence in warm climates & people of all races,
sexes & ages are subjected to infection.
Mode of transmission by:
1) Contamination of water with viable cyst.
2) Person-to-person contact.
3) Food handler’s.
4) Filth flies.
Control
1) Treatment of patient.
2) Screening of food handlers & treat the infected cases.
3) Improvement of hygiene & sanitation.
4) Human excreta must be disposed properly.
Unit 2: Protozoa
10
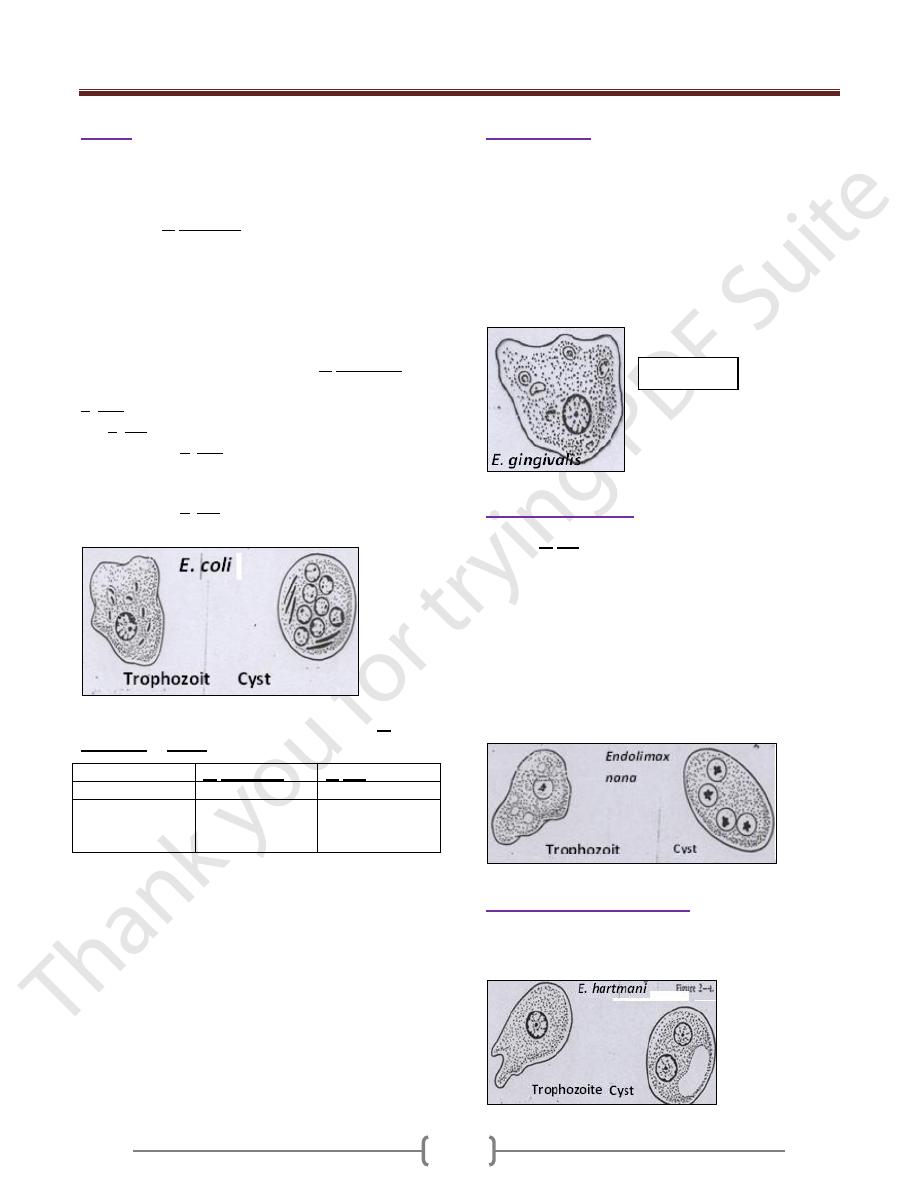
E.coli
The most common amoebic parasite of man (commensal).
It habits large intestine.
It has trophozoite & cyst stages, both of them are larger
than those of E. histolytica. The trophozoite size is (15-
50) µ, no RBCs seen in food vacuoles. There is no sharp
point between ectoplasm & endoplasm in trophozoite
stage.
In cyst stage (its size 10-33 µm), the mature cyst contains
8 nuclei, each of them has same feature of trophozoite
nuclei.
The shape of chromatoidal bodies in of E. histolytica is
cigarette, rounded in shape, but it is needle shaped in the
E. coli if presented.
The E. coli is not parasitism but commensalisms.
The presence of E. coli in stool of some bodies means the
food of this patient contaminated with feacal material,
how? By the Musca domestica, filth fly, or others.
The presence of E. coli in the host means his food been
contaminated.
There are 2 things for differentiation between E.
histolytica & E. coli
The difference
E. histolytica
E. coli
Karyosome
Central
Eccentric
Chromatin line
nuclear
membrane
Fine & regular
distributed
Course &
irregular
distributed
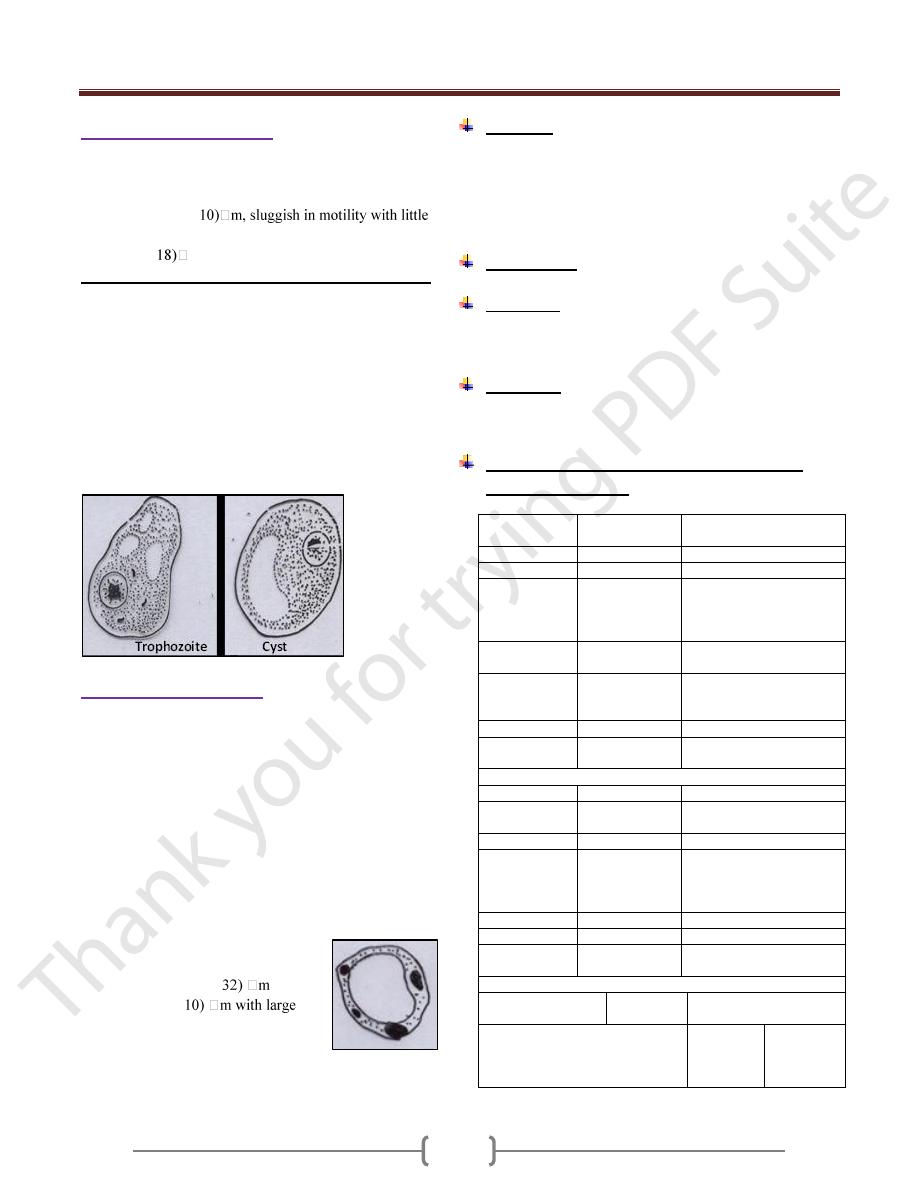
E.gingivalis
Only trophozoite been reported in E. gingivalis .
The size of the trophozoite is (15-30) µm.
It is nonpathogenic but opportunistic (in diseased gum or
tonsils).
The karyosome is central or somewhat eccentric.
It is found in diseased gum & tonsillitis as a phagocytic
(opportunistic).
It is transmitted through saliva droplets or intimate contact.
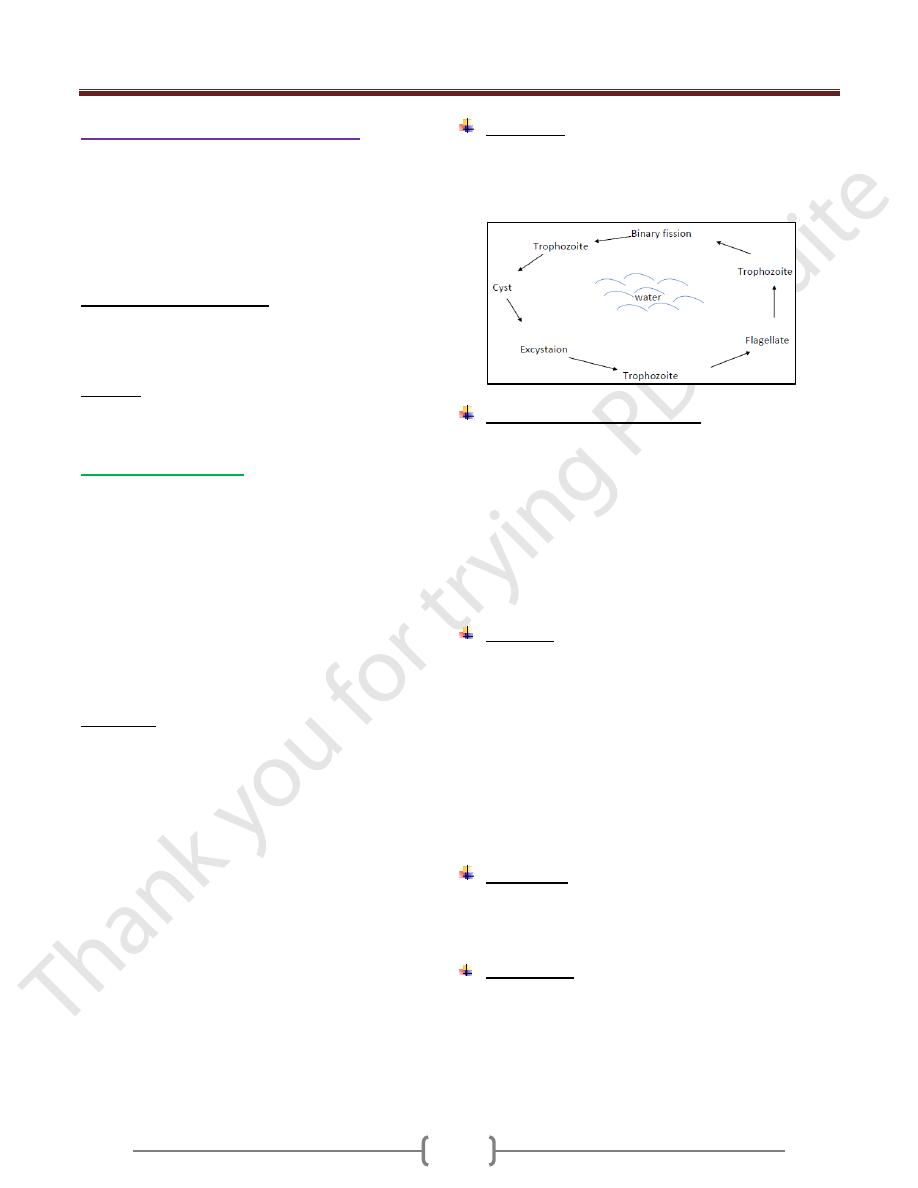
Endolimax nana
Like the E. coli, its presence means the food of the person
been contaminated with stool (feacal matter) of other person
It has trophozoite & cyst stages. The trophozoite has one
nucleus, and the cyst has 4 nuclei. The karyosome
consisting from one or more granules, commonly
eccentric in position.
The size of the trophozoite is (8-10) mm, the endoplasm
finally granular with numerous vacuoles.
In the cyst chromotoidal bodies, if present are short
curved rods or comma shaped.
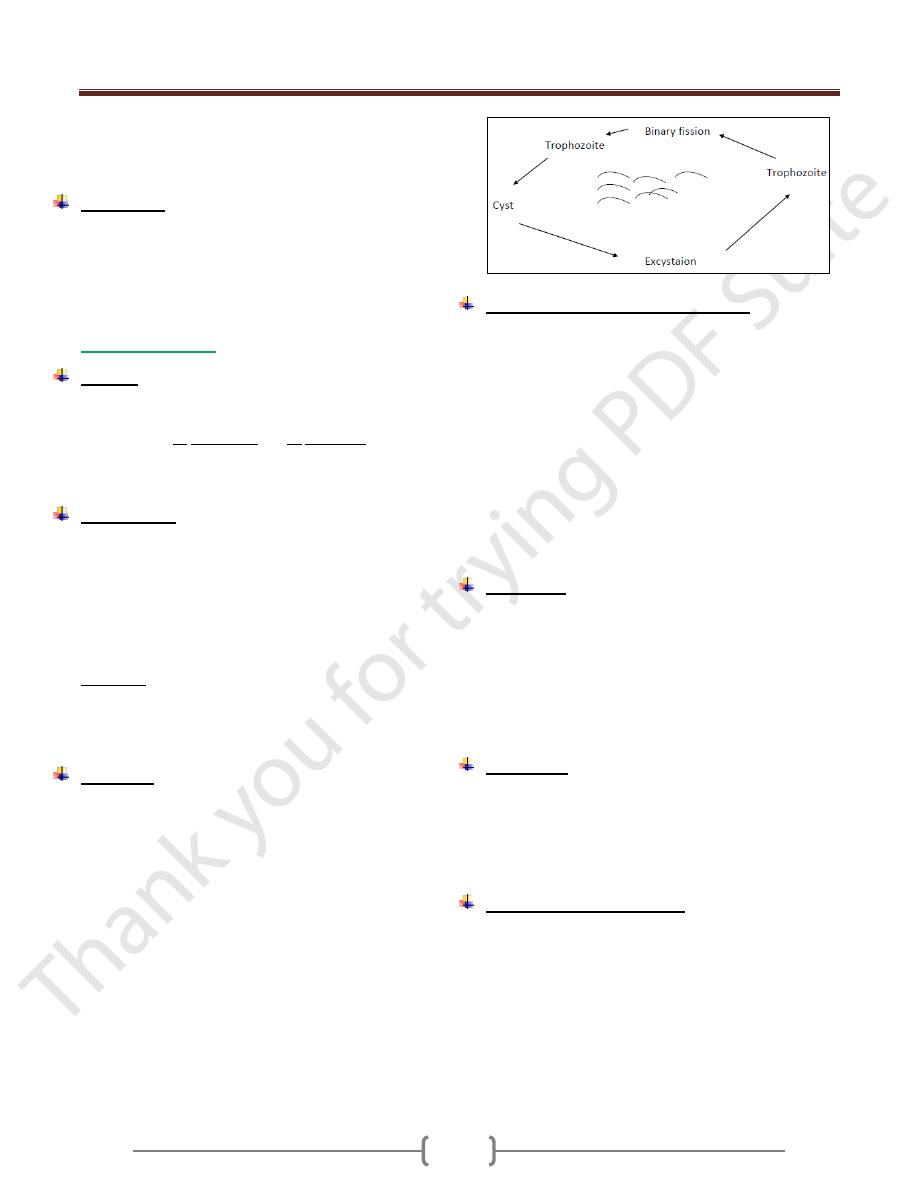
Entamoeba hartmanni
Small race of E. histolytica, sometimes it is mistaken with
E. nana, fortunately both of them are nonpathogenic.
Trophozoite
Unit 2: Protozoa
11
Iodamoeba buetschlii
Cosmopolitan, commensal, living in lumen of large intestine
It has 2 stages:
Trophozoit: (8-
evidence of pseudopodial extensions.
Cyst: (5-
m.
We can differentiate between I. buetschlii & others by:
The trophozoite & cyst have one nucleus & both of them
have glycogen vacuoles, so in stain with iodine to give
brown mass.
A large karyosome in nucleus found centrally or
somewhat eccentrically.
Only the trophozoite of this amoeba has one or two
distinct glycogen vacuoles.
The cyst has only one nucleus, it has large glycogen
vacuoles which stained with iodine in deep brown color.
So these differences are very important.
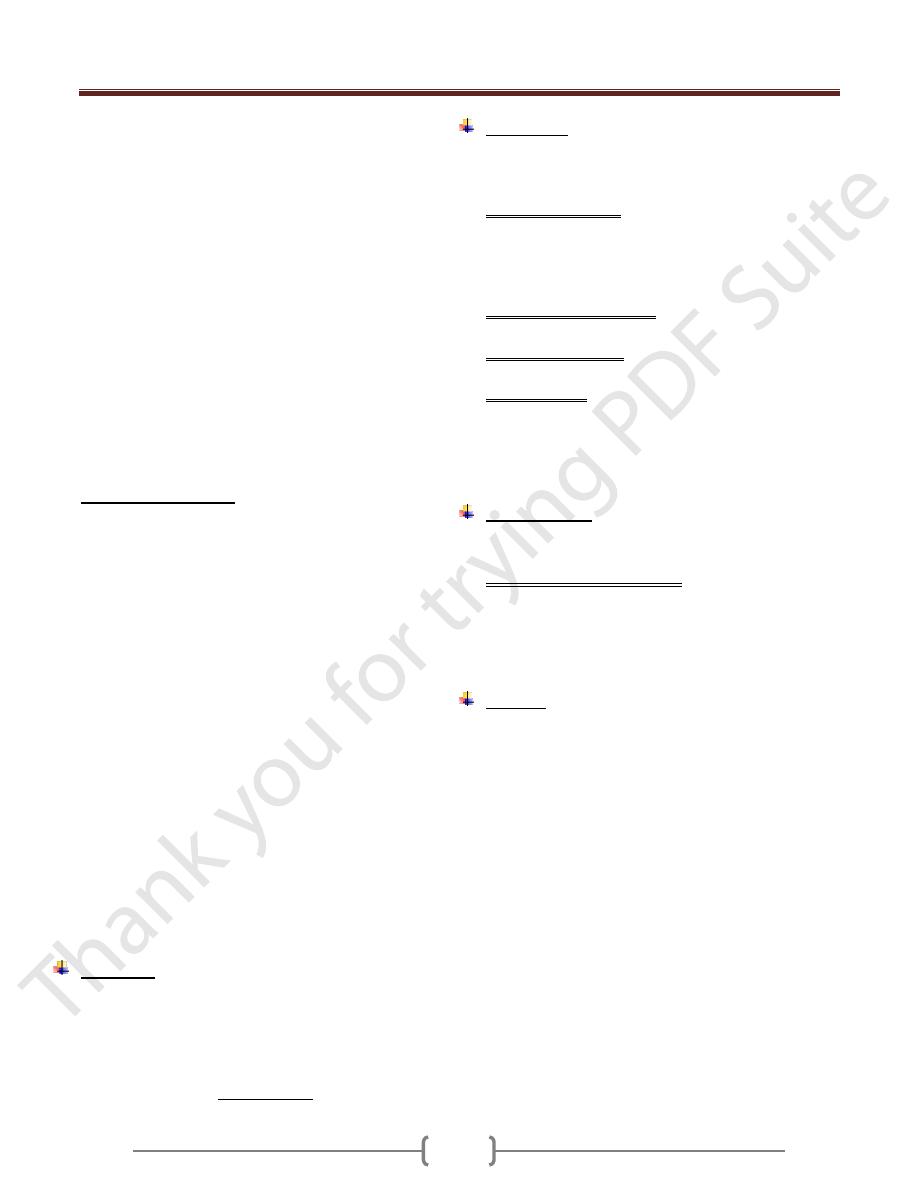
Blastocystic hominis
It is parasitic amoeba.
Discovered in 1912.
Its life cycle is not clear.
Since discovered, B. hominis has been the subject of
controversy, initially described as algae, them as harmless
intestinal yeast, and since around 1982 as a protozoan
parasite.
Although a number of different forms of it are known, so
only vacuolated form is more common & easy to
recognize, therefore only this form is described.
The different form of B. hominis:-
1) Vacuolated type, which is the
most common type.
The size range from (5-
, but
the average is (7-
vacuole in the center forming about
10% at the periphery with 4 nuclei
situated at same level.
2) Granulated type.
3) Amoeboid type.
Life cycle
The life cycle has not been universally described, but it
may participate in a sexual reproduction.
Main method of reproduction is by binary division &
sporulation & it transmitted through contaminated food &
water, and it is prevalent in tropical & subtropical areas.
Pathogenesis
Is not well known & need to be determined.
Symptoms
Mainly diarrhea, nausea, vomiting, fever, as well as
abdominal pain & cramps.
Treatment
The best drug of choice is a combination of Flagyl &
Septrin
Essential differences between bacillary &
amoebic dysentery
Bacillary
dysentery
Amoebic dysentery
Number
> 10 per day
(6-8) per day
Amount
Small
Relatively copious
Appearance
Consist of
blood & mucus,
hardly any
faecal matter
Feces with stratum of
blood & mucus seen over
the surface
Color of
blood
Bright red
(fresh blood)
Dark red
(latered blood)
Consistency
Viscid, mucous
adherent to
container
Liquid or formed, mucus
not adherent to container
Odor
Odorless
Offensive
Chemical
reaction
Alkaline
Acidic
Microscopic examination
Pus cells
Numerous
Scanty
Red blood
cells
Discrete
In clumps, discolored
Eosinophils
Absent or rare
Present
Macrophages
Present
showing
ingested
erythrocytes
Absent
CL crystals
Absent
Present
E. histolytica
Absent
Trophozoites Present
Bacteria
Scanty, non-
motile
Numerous & motile
Cultural examination
Growth on media
for E. histolytica
Negative
Trophozoites grown
Growth on MacConkey agar
Positive
for
Shigella
spp.
Negative
Unit 2: Protozoa
12
Pathogenic free living amoebae
Free –living organisms that are capable of adapting to a
parasitic existence are called amphizoic. Meaning that
they can multiply both in the body of the host (endozoic)
and in free living (exozoic) condition.
Species of the two general Naegleria and Acanthamoeba
are among such organism
Geographical distribution:
Infection with free living amoebae was first discovered in
1965, in Australia, USA them in Europe, Africa, Asia,
newzealand.
Habitat:
in fresh water (lakes, ponds), Sea water,
sewage water, brackish water.
Naeglaria fowleri:
Causes, primary amebic meningoencephalitis (PAM)
which produces death within 5-7 days after the onset of
symptoms
Most cases have occurred during the hot summer months
in young people who within the preceding week swam or
dived in fresh or brackish water, lakes streams, hot
springs also, swimming pools have been apparent source
of the infection, few cases by inhalation of infected dusts
are also recorded
Portal of entry to the brain and meninges found to be the
nasal mucusa and cribiform plate.
Morphology, Naegleria fowleri, live well in fresh water
and moist soil, also grows well in tissue culture and
artificial media.
Occurs in trophozoite and cyst forms Motile trophozoites
from cerebrospinal fluid are elongate, broad anteriorly,
with single broad pseudopod at the forward end, the size
around 7 by 20 Micro meters, one nucleus with a large
central karyosome (endosome).
When the species is transferred to water, contractile
vacuoles become evident and flagellate forms with two
flagella begin to appear among ameboid forms.
The ameba flagellate forms are a transient forms , pear in
shape with two flagella at its broad , anterior end , they
moves rapidly forward or spin slowly in a circle ,
Under adverse circumstances it converted into cystic form
, which are spherical with a smooth thick wall ,
uninucleate and 7 to 10 Micro meter in diameter .cyst are
not formed in the tissue ,
Life Cycle
The amoebae invade the nasal mucosa; pass through the
olfactory plate into the meninges.
Multiplication is by binary fission, there is no sexual stages,
mitosis occurs and the nuclear membrane is retained.
Pathogenesis and symptoms
The amoeba colonize the nasal tissue and connected
sinuses and through the olfactory nerves into the brain.
At autopsy, the affected areas of the brain are soft, and the
meninges are congested and purulent. In tissues sections
the parasite found in the perivascular tissues where the
inflammatory cells are few or absent.
The symptoms of the disease are those of bacterial
meningitis such as frontal headache, high fever nausea,
vomiting, vision problems and mental problems.
Diagnosis
A history of exposure to stagnant or thermal water (springs)
3-6 days before the onset of symptoms of meningitis or
meningoencephalitis suggests the infection with naegleria.
In unstained wet preparation the trophozoite amoeba can
be recognized by their motility.
While they are recognized with difficulty in gram
negative or wright stained smears.
Culture isolation from cerebrospinal fluid or tissues can
be attempted on a plate of 1.5% non-nutrient agar seeded
with living Escherichia coli.
Treatment
To the few survived people amphotericin B & miconazole
was given intravenously and intra thecally, rifampin orally
& sulfisoxazole intravenously was found to be useful.
Epidemiology
PAM is a relatively rare disease with worldwide in
distribution ,infections where acquired while swimming
,diving with fresh water lakes, ponds, streams, warmed by
industrial effluent ,or natural thermal springs.
N. fowleri grows well at high temperature and tolerate
temperature up to 45° C.
Unit 2: Protozoa
13
Although cysts in air-borne dust are a theoretical source
of infection, but the trophozoite stage taken into the nose
in water is usual infective source.
Prevention
The best protective measure is to avoid exposure in warm
natural water, especially thermal springs, streams and
adequate chlorination of public water supply including
swimming pools.
Acanthamoeba
Disease:
Granulomatous amoebic encephalitis, uveitis, corneal
ulceration. Several species are considered pathogenic to
human such as A. culbertsoni and A. castellanii.
It causes a chronic disease which may last for more than a
week or even monthes before causing death.
Morphology
Acanthamoeba active trophozoite (12-45 µm) in diameter
and has irregular shape with spine-like pseudopodia called
acanthopodia arising from lobopodia and other areas of
the body
There is no flagellate form, contain one nucleus,consisting
of a large karyosome. No peripheral chromatin granules,
the cytoplasm appears granular and vacuolated.
Cyst stage: spherical (8-25 µm) with double wall forming
a smooth wrinkled outer wall (ectocyst) and a stellate or
roughly polygonal inner wall (endocyst).the single
nucleus is similar to that of trophozoite.
Life cycle
Infection can be acquired by inhalation, ingestion or
through traumatized skin or eyes. CNS infection is not
associated with swimming. invasion of CNS is secondary
to infection elsewhere in the body, Amoeba reach the
brain by the way of the blood stream from the lower
respiratory tract or through skin or mucosa.
A rapid transformation from cyst to trophozoite in the
nasal mucosa with subsequent CNS involvement.
Direct invasion of the eye are contracted in persons who
swim in ponds water with their contact lenses in place.
Improper cleaning of the lenses after their removal allows
the trophozoite to grow and multiply.
The trophozoite attach to the contact lenses after
reinsertion of the lenses. The trophozoite invades the eye
and digests corneal epithelial cells.
Pathogenesis and symptomatology
Invasion of the brain occure in chronically ill and
immunosuppressed patients. When the primary site of
invasion is the skin the onset of CNS symptoms comes
several month to a year later, the symptoms include
headache, sore throat, fever, neck stiffness, seizures,
nausea and vomiting. Cyst and trophozoite found in the
granulomatous lesions of the brain.
The lesions also found in skin, kidney, liver, lymph nodes,
ear, heart, prostate and eye.
Infection of the cornea of the eye (amoebic keratitis)
caused severe ocular pain and vision problems.
Penetration of the cornea may result in loss of vision.
Diagnosis:
The specimen of choice for diagnosing of trophozoite and
cyst is CSF also brain tissue, corneal scrapings and
suspected scraping may be cultured on agar plates seeded
with gram negative bacteria then transferred to a liquid
broth containing antibiotics.
Special (immunoenzymatic) staining of formalin fixed
tissue may be useful.
Treatment
No satisfactory GAE treatment available. Most patients
died before any diagnosis or treatment. Cases of
Acanthamoeba keratitis has been treated with a
combination of Neomycin drops, dibromopropamide
ointment and Brolene.
Epidemiology and control
Saurce of infection was presumed to be dust or water.
Infection found in people who are immunocompromised
or contact lenses wearer. Poor hygiene practice such as
using home made saline or tap water as rinsing solution
are major risk factor that may lead to infection.